
Abstract
BACKGROUND AND PURPOSE: Percutaneous cement augmentation has been reported as an effective salvage procedure for frail patients with spinal instrumentation failure, such as screw loosening, hardware breakage, cage subsidence, and fractures within or adjacent to stabilized segments. Favorable results were reported during a median follow-up period of 16 months in a retrospective analysis of 31 consecutive procedures performed in 29 patients. In the present study, the long-term effectiveness of this treatment in avoiding or postponing revision surgery is reported.
MATERIALS AND METHODS: Clinical and radiologic data of our original cohort of patients were retrospectively collected and reviewed to provide an extended follow-up assessment. The need for revision spinal surgery was assessed as the primary outcome, and the radiologic stability of the augmented spinal implants was considered as the secondary outcome.
RESULTS: An extended radiologic follow-up was available in 27/29 patients with an average of 50.9 months. Overall, 18 of 27 (66.7%) patients, originally candidates for revision surgery, avoided a surgical intervention after a cement augmentation rescue procedure. In the remaining patients, the average interval between the rescue cement augmentation and the revision surgery was 22.5 months. Implant mobilization occurred in 2/27 (7.4%) patients; rod breakage, in 1/27 (3.7%); a new fracture within or adjacent to the instrumented segment occurred in 4/27 (14.8%) patients; and screw loosening at rescued levels occurred in 5/27 (18.5%) patients.
CONCLUSIONS: In this cohort, cement augmentation rescue procedures were found to be effective in avoiding or postponing revision surgery during long-term follow-up.
ABBREVIATION:
- ASA
- American Society of Anesthesiologists
SUMMARY
PREVIOUS LITERATURE:
Cement augmentation has been shown to be a potential alternative to revision surgery in the short term for fragile and elderly patients with spinal implant failures or new fractures. A recent systematic review of case series on cement rescue augmentation by Cawley et al9 included studies with a median follow-up of 12 months, suggesting that cement augmentation in selected patients can help in stabilizing loosened screws and treating vertebral fractures.
KEY FINDINGS:
The present study, with an average follow-up of 50.9 months, found that 66.7% of patients avoided surgery, and for those who required revision surgery, it was postponed by an average of 22.5 months. This delay could significantly improve quality-adjusted life years for patients with low life expectancy.
KNOWLEDGE ADVANCEMENT:
The extended follow-up period in this study demonstrates the long-term efficacy of percutaneous salvage procedures, establishing cement augmentation as a practical and less invasive alternative to avoid or postpone revision surgery for selected and fragile patients.
Instrumented spinal surgery is widely used in the treatment of degenerative, traumatic, and neoplastic pathologies of the vertebral column. As patients undergoing spinal surgery increase in age, concurrent osteoporosis has become a frequent comorbidity and is one of the main causes of spinal instrumentation failure. Bone mineral density of the spine has been shown to affect the stability of pedicle screws,1,2 with loosening in up to 25% of patients with reduced bone mineral density.3 The length of the stabilization,4 sagittal and frontal imbalance, and thoracic localization are further factors influencing the stability of the spinal constructs.5 In addition to bone resorption and screw loosening, cage subsidence and fractures both in the instrumented segment and at junctional levels represent the most common delayed causes of instrumentation failure. These occurrences are often associated with recurrent pain and may require revision surgery.6,7 Revision surgery remains the criterion standard for implant failure, but it is associated with further potential morbidity and increased costs.8 Moreover, revision surgery may not be suited for patients with severe comorbidities, in whom such a procedure, often more invasive than the index operation, may represent a significant risk. Accordingly, percutaneous cementation has been reported as a salvage procedure for this elderly and frail patient group and may represent a safe and effective alternative to surgical revision.9⇓–11
Our group has previously reported on cement augmentation in the treatment of clinically relevant implant failure in a retrospective analysis of 31 consecutive procedures performed in 29 patients, with favorable results found during a median follow-up period of 16 months.12 Subsequent publications from other centers have reported similar observations in terms of the feasibility and safety of cement augmentation in frail and elderly patients,11,13⇓–15 even in complex instrumentation cases such as intervertebral body implant failure.16 A recent systematic review has been published on salvage cement augmentation in cases in which surgical revision is not considered a viable option.9
It is, however, not yet known whether these favorable outcomes remain sustained in the long-term. To address this question, we conducted an extended follow-up study based on a retrospective analysis of medical records of our original patient series.
MATERIALS AND METHODS
General Methods
In our previous study, 29 patients were treated between May 2013 and October 2016 with rescue cement augmentation for clinically relevant screw loosening with bone resorption, cage subsidence, and vertebral fracture within or adjacent to the instrumented segments. Instrumentation failure was deemed clinically relevant if associated with new or recurrent pain correlated with imaging findings or if deemed a threat to spinal biomechanical stability. Indications for primary spinal instrumentation included traumatic, degenerative, and neoplastic conditions.
We retrospectively collected and reviewed all available clinical and radiologic data related to any spinal interventions until November 2023, defined as extended long-term follow-up.
The details of the rescue procedures were described in the original study, which included 13 procedures with cement augmentation of fractures within or adjacent to the instrumented segment, 9 procedures with augmentation around loosened screws, and 8 with both. One procedure was aborted.
Informed consent was obtained from all patients. The local ethics committee approved this retrospective study.
The primary outcome assessed in this long-term follow-up study was the effectiveness in avoiding or postponing revision spinal surgery at the previously instrumented spinal segment or at adjacent levels following the cement augmentation rescue procedure. The time interval between the cement augmentation and the revision surgery as well as the indication and the type of new surgical intervention were also recorded. The American Society of Anesthesiologists (ASA) physical status classification system was adopted as a general indicator of patients’ physical statuses.
The secondary outcome was the radiologic outcome of the previous cement augmentation procedures and implant stability assessment based on long-term imaging follow-up performed for the index spinal pathology or for unrelated reasons. The duration of radiologic follow-up was defined as the time between the original rescue procedure and the last available imaging follow-up.
Long-term imaging follow-up consisted of conventional radiograms, CT scans, and MRI studies including the spinal segment of interest.
The radiologic images were reviewed by a neuroradiologist and a neurosurgeon in consensus, defining the radiologic outcome of the previous percutaneous cement augmentation procedures in terms of implant mobilization and integrity, further cage subsidence, new fractures, or spinal deformity. For patients with an available CT scan, onset or progression of screw loosening was also recorded.
Statistical Methods
Characteristics of all included patients are described as mean (SD) or median and first and third quartiles and as count and percentage. Follow-up data are described as count and percentage. The Kaplan-Meier method was used to compute the cumulative probability of being free from revision surgery (ie, “avoided surgery”) for >4 years of follow-up. Patients who remained free from surgery were censored at the last follow-up time.
RESULTS
Basic characteristics of the study population are summarized in Table 1. An extended follow-up was available in 27/29 patients: male/female ratio: 10/17; age range at time of the original treatment: 50−82 years; average age: 71.3 years. For 1 patient an extended follow-up was not recorded because the rescue procedure was aborted due to technical reasons, while another patient moved abroad and no follow-up data could be collected. The median follow-up time of our cohort was 54 months (first quartile: 21 months; third quartile: 78 months).
Baseline characteristics of the population
Seventeen of 27 patients were still alive at the time of medical record analysis, while 10/27 had died due to causes unrelated to the spinal pathology and to the cement augmentation (3 cases of oncologic progression, 3 cases of acute coronary syndrome, 2 cases of trauma, 1 case of COVID-19, and 1 case of sepsis unrelated to spinal surgery and intervention). Fifteen of 27 patients were identified as “ASA 2,” and 12/27 patients were identified as “ASA 3.”
An extended radiologic follow-up was available for 27 patients, with an average of 50.9 months at the last imaging study (range, 2–103 [SD. 32.2] months). In 16 patients (59.3%), follow-up imaging was available beyond 4 years.
Overall, the instrumentation was in the thoracic segment in 1/27 patients, in the thoracolumbar segment in 16/27 (Fig 1), and in the lumbosacral segment in 10/27 (Fig 2). There was no significant correlation between the instrumented segment and the need for revision surgery. The average length of the instrumentation was 5.7 levels (range, 2−14 levels). Available follow-up imaging was a CT scan in 17 patients, an MRI scan in 2 patients, a conventional radiograph in 6 patients, CT + MRI in 1 patient, and CT and conventional radiographs in 1 patient.

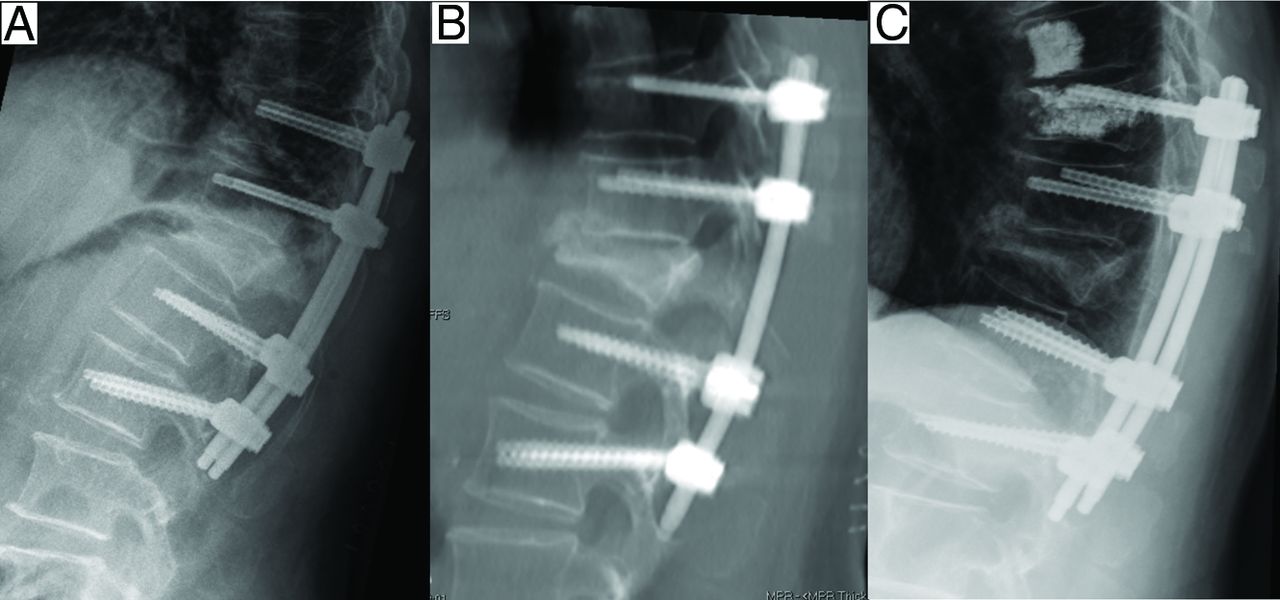
Standing lateral radiograph (A) of a 76-year-old patient with T10–L2 posterior fixation and decompression for treatment of a burst vertebral body fracture of T12 with posterior wall retropulsion and central canal stenosis. Sagittal thick-layer MPR reconstruction from a CT scan (B) shows a new fracture of T10 with initial “pullout” of the screws 1 month after surgery. The patient was treated with rescue cement augmentation on the fractured vertebral body and prophylactic augmentation at the level above. Standing lateral radiograph (C) performed 3 months after the rescue augmentation shows stability of the treatment. The patient was followed up to 85 months after surgery, and no further invasive procedure was needed.

Standing lateral radiograph (A) of a 57-year-old patient with T12-S1 posterior fixation and decompression for treatment of a multilevel central canal stenosis. CT axial image (B) shows bilateral screw loosening at S1, deemed symptomatic. Intraprocedural fluoroscopy (C and D) of a rescue cement augmentation procedure performed bilaterally at S1. CT axial image (E) and radiograph (F) follow-up after 20 months show stability of the construct. Patient improved clinically after the augmentation rescue procedure, and no surgical intervention was necessary.
During the extended follow-up interval, imaging revealed implant mobilization in 2/27 (7.4%) patients and rod breakage in 1/27 (3.7%), and a new fracture within or adjacent to the instrumented segment occurred in 4/27 (14.8%) patients. Fractures were located at the adjacent segments in 2 patients, within the instrumented segments in 1 patient, and in both the adjacent segments and within the instrumented segment in 1 patient. Among patients with a CT scan during the extended follow-up interval, screw loosening in rescued segments was observed in 5/19 patients. No further cage subsidence or new relevant spinal deformity occurred.
Overall, 9 patients needed revision surgery at the instrumented segment or adjacent levels. The average time interval between the rescue cement augmentation and the revision surgery was 22.5 months (range, 2−47 months).
Reasons for revision surgery were adjacent segment degeneration in 3/9 cases, screw loosening in 1/9 cases, both implant mobilization and new fracture in 1/9 cases, both screw loosening and implant mobilization in 1/9 cases, and infection in 1/9 cases. In 2/9 cases, reasons for revision surgery were unknown (surgery performed at other centers).
Among the 9 patients requiring a surgical revision, 2 were treated with extension of the instrumentation due to adjacent segment degeneration; 3, with implant removal; and 3, with both implant removal and extension of the stabilization. One patient treated at another center with implant removal also underwent cement augmentation for a new vertebral fracture within the instrumented segment. One patient underwent multiple unspecified revision procedures at different hospitals abroad. The new fractures were treated in 2/4 cases with cement augmentation vertebroplasty, associated with implant removal in 1 case due to implant mobilization. A conservative approach for the remaining 2 fractures was adopted.
Overall, the probability of being free from revision surgery following the cement augmentation rescue procedure was 79.6% at 3 years (95% CI, 64.8% to 97.7%), despite originally being candidates for revision surgery (Fig 3).

Kaplan-Meier curve with 95% CI band and an at-risk table.
In the subgroup of patients who did not undergo revision surgery, the average length of instrumentation was 5.3 levels, while it was 6.4 levels for patients who underwent revision; the difference was not statistically significant.
The main results are summarized in Table 2.
Technical information regarding the procedures
DISCUSSION
Rescue cement augmentation in selected fragile patients with implant failure or new fractures after spine surgery may represent a safe and effective technique to avoid or postpone revision surgery: On an average follow-up interval of 50.9 months after a rescue augmentation, 66.7% of patients in our series had avoided surgery, and for those who required revision surgery, the intervention was postponed for almost 2 years (22.5 months).
Revision surgery remains the first treatment option for symptomatic implant mobilization, with the aim of easing pain and ensuring the stability of the posterior fixation.17 The surgical treatment is also useful in collecting material for microbiological analysis to provide information regarding low-grade infection, which is present in up to 29% of cases with implant mobilization.18,19 On the other hand, conservative management is an option in asymptomatic patients.20 Surgical treatment usually involves implant removal and replacement using larger screws (a 2-mm increase in diameter significantly enhances the resistance to pullout17) using allograft bone21 or cement22 with or without prolongation of the stabilization. Because the anatomy can be distorted and scar tissue is present, these revision surgeries are usually more invasive, last longer, and come with a higher risk of complications23,24 compared with index surgeries.
Cement augmentation techniques may, therefore, offer an alternative option to surgery in fragile patients. Their aim is to stabilize loosened screws and mobilized implants and treat vertebral body fractures within the fixation segment or at the adjacent levels, with the aim of avoiding or at least delaying revision surgery in patients in whom open surgery is deemed dangerous or too invasive. Of note, cement augmentation has been demonstrated as not being inferior to revision surgery from a biomechanical perspective.25 Our results seem to align with the biomechanical characteristics of cement salvage, considering that no new deformities were observed during our long-term follow-up.
Our original patient cohort presented with clinically relevant screw loosening with bone resorption, cage subsidence, or vertebral fractures within or adjacent to the instrumented segments and had a surgical indication, either due to the biomechanical situation or because of pain symptoms, yet these patients were not considered good surgical candidates. It is conceivable that without a minimally invasive possible solution at hand, such as cement augmentation rescue, some of them would have been managed conservatively.
Because of their general conditions and/or advanced age, rescue cement augmentation was found to be indicated instead of surgical revision after a multidisciplinary spine board discussion with spine surgeons, neuroradiologists, and pain physicians.
Our follow-up interval (50.9 months on average) is longer than that of other studies published to date. In a recent review by Cawley et al9 that included our previous report and 10 other studies regarding cement augmentation, a median follow-up period of 12 months was reported (average 12.1 months; range, 3−24 months). Of the 27 patients included in our cohort, a total of 9/27 patients required revision surgery.
The most common reason to repeat surgery was adjacent segment degeneration (3/9). Infection was the indication in another patient (1/9). One patient (1/9) underwent a repeat operation due to screw loosening; another (1/9), due to implant mobilization; and another (1/9), due to both screw loosening and implant mobilization. Two patients underwent an operation in other centers and revision surgery for unknown indications. For 1 of these 2 patients, the type of surgery is also unknown, while the second patient underwent implant removal, extension of the stabilization, and cementoplasty for an adjacent segment vertebral body fracture. Two of 9 patients subsequently underwent an operation in our center with implant removal and extension of the stabilization, while 3/9 underwent implant removal only, and 2/9, extension of the stabilization only.
Vertebral fracture at the level of the loosened screws or adjacent to the instrumented segments is a well-known complication for which percutaneous vertebroplasty has been already described as a treatment option.26 In a total of 4/27 of our patients (14.8%), a new fracture was diagnosed within the instrumented levels (2 patients), at a junctional level (1) or both (1). To treat the new fractures, a cementoplasty was performed in 2 cases and a surgical intervention in 1 case; in the last case, no further treatments were performed due to lack of symptoms.
The fragility of our population is highlighted by the finding that >1 of 3 patients (37%, 10/27) died during the extended follow-up period due to causes unrelated to the surgery or the cement augmentation. Among the patients who required a surgical revision after rescue cement augmentation, the median time between cement augmentation and the new surgical intervention was 22.5 months. Delaying surgical treatment for a few months or years may be beneficial in terms of quality-adjusted life years, or it may be helpful to entirely avoid surgery in patients with a low life expectancy.
The present study lacks clinical outcome scores; this is in contrast with our previous work in which clinical outcome had been reported.12 Our previous results, in line with Wang et al,13 demonstrate that rescue cement augmentation favorably impacts short-term clinical outcome. In the present study, clinical scores such as the Numerical Rating Scale pain scale were not reported because patients were no longer being routinely followed at that point, for some patients several years after their procedures. Moreover, pain scores may not be a reliable outcome parameter because they may well reflect the wider influence of patients with failed back surgery; also, the association between the procedure and the clinical outcome may be difficult to assess after 10 years postprocedure. Our clinical end point was, therefore, the need for revision surgery, which, in our opinion, is a more relevant clinical variable.
Other limitations of our study are its retrospective analysis, the absence of sagittal balance measurements and DEXA scores, and the lack of a control group.
A prospective randomized trial (revision surgery versus rescue cement augmentation versus conservative management) would be ethically questionable and difficult to perform due to the fragility of these patients together with the variable complexity of biomechanical, clinical, and surgical aspects.
CONCLUSIONS
Cement augmentation performed to salvage spinal hardware failure allowed avoiding or delaying revision surgery during long-term follow-up in a large proportion of frail patients in our cohort, in whom revision surgery would have a significant risk of morbidity. The indication for cement salvage procedures should be reached after multidisciplinary discussion and tailored to the requirements of individual patients who present with a higher surgical risk.
Footnotes
F. Polinelli and M. Pileggi share first co-authorship.
A. Cardia and A. Cianfoni share last co-authorship.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received February 23, 2024.
- Accepted after revision June 21, 2024.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.