
Abstract
Summary: Embolization of a carotid cavernous fistula (CCF) by means of a detachable balloon is an established method for treating CCFs while preserving a patent parent internal carotid artery (ICA). However, failure to embolize the CCF may occur on a few occasions, such as when the balloon cannot pass through the fistula into the cavernous sinus by blood flow, or when the inflated balloon in the cavernous sinus retracts to the carotid artery. Under these circumstances, the ICA may have to be sacrificed in order to treat the CCF. Herein we describe a double-balloon technique for embolization of a CCF. By applying this technique, we successfully treated nine of 11 CCFs, without compromise of the parent ICA when the conventional one-balloon technique failed.
Carotid-cavernous fistulas (CCFs) are classified into four types, according to Barrow DL et al (1). Type A is defined as a direct shunt between the intracavernous portion of the internal carotid artery (ICA) and the cavernous sinus (CS). It is usually and simply called a CCF or the direct type of CCF. Types B to D are indirect shunts, often attributable to dural arteriovenous fistulas or dural arteriovenous malformations of the CS. In this report, we focus on the type A CCF.
Embolization of a CCF by means of a detachable balloon has been widely accepted as a therapeutic option (2–8). Ideally, the parent ICA can often be preserved with this technique. However, Lewis et al reported that, when using a detachable balloon, carotid blood flow was only preserved in 75% of their patients (9). Failure to embolize the CCF from the arterial approach, using a detachable balloon, may occur on a few occasions, such as when the balloon cannot pass through the fistula into the CS by blood flow, or when the inflated balloon in the cavernous sinus retracts to the parent ICA.
In order to solve these dilemmas, we have developed a double-balloon technique that may increase the success rate in the embolization of CCFs by preserving blood flow in the parent ICA.
Technique
During the past 3 years (from March 1996 to February 1999), 31 consecutive CCFs were treated at our institution (Table). Two CCFs were recurrent after previous surgical trapping. The other 29 fistulas, which were not treated previously, had patent ICAs. In all 29 CCFs with patent ICAs, we started embolization by using one detachable balloon from the arterial approach, and tried to preserve the parent ICA. Debrun's N3 detachable balloon set was used. A 9F guiding catheter was placed in the cervical ICA. A detachable balloon was mounted at the tip of the 2F catheter in the 2/3F coaxial catheter system. The size of the balloon to be used was determined on the basis of the size of fistula and CS on the angiograms. The balloon was advanced to the ICA inside the 9F guiding catheter to explore the opening of the fistula. After passing through the fistula, the balloon was inflated on the venous side (CS) to occlude the fistula. A rotating Y-connector with adjustable valve (Microvena Corp., MN) or a double-rotating Y-connector with adjustable valve (Microvena Corp.) was used to prevent blood oozing between the 9F guiding catheter and the 2/3F coaxial system.
Cases of CCF, March 1996 to February 1999 (n = 31)
If the detachable balloon failed to be located in the CS, we proceeded to apply the double-balloon technique in which one more balloon catheter was used to facilitate placement of the embolization balloon.
We discovered that this technique was helpful in the following two circumstances. First, the exact site of the fistula could be identified by a sump effect, with the partially inflated balloon staying at the orifice of the fistula, but the balloon could not be carried to the venous side through the fistula by blood flow (seven cases). Second, the single detachable balloon could pass through the fistula, but retracted to the ICA after inflation (two cases).
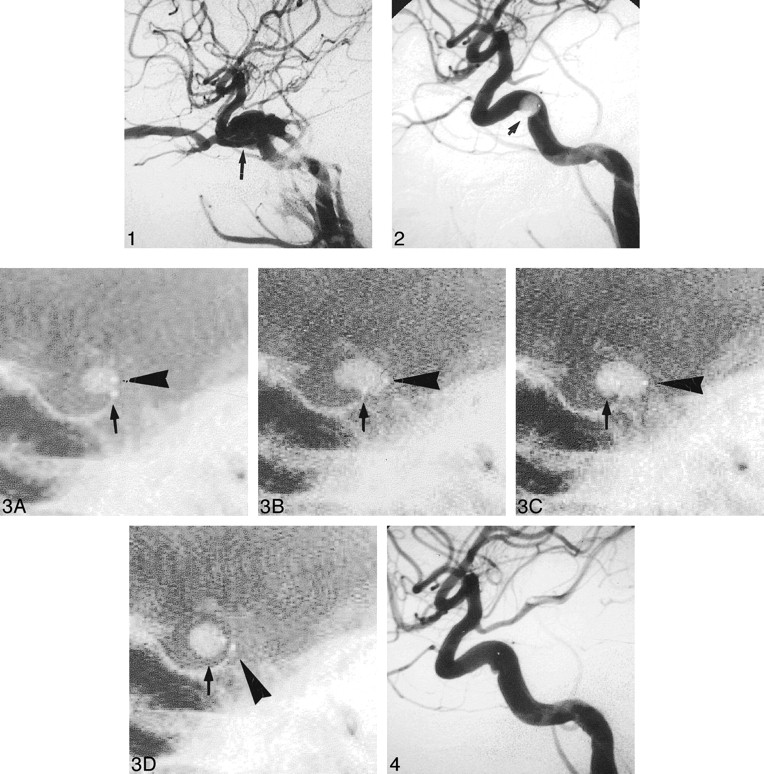
For the first situation mentioned above (Fig 1–4), the procedure was described as follows. Step 1. The first balloon (the embolization balloon) to be placed inside the CS was brought to the orifice of the fistula and was inflated to a size that would stay at the orifice of the fistula. Step 2. The second balloon (the bracing balloon) was inflated in the ICA, overlying the embolization balloon. The bracing balloon was inflated to a size so it would not be moved or detached by subsequent inflation of the embolization balloon. Step 3. The embolization balloon at the fistula was deflated and then inflated. With the bracing balloon occluding the lumen of the ICA, the embolization balloon would usually pass through the fistula to the CS in the direction of least resistance. Step 4. Inside the CS, the embolization balloon could slowly be inflated to a proper size to obliterate the fistula. Step 5. The bracing balloon was then deflated and retreated away from the orifice of the fistula. Step 6. A control angiogram was performed. Step 7. The size of the embolization balloon was further adjusted if necessary; then, the embolization balloon was detached. Step 8. The bracing balloon catheter was removed.

Lateral-view right carotid angiogram shows carotid cavernous fistula (arrow).fig 2. A balloon (arrow) is sucked to the fistula in the ICA. However, it cannot pass through the fistula to enter the CS. This is the first indication for using the double-balloon technique.fig 3. Steps involved in double-balloon technique. The embolization balloon marked by an arrow is to remain inside the CS after embolization. The bracing balloon, indicated by an arrowhead, is for temporary inflation inside the carotid artery, and will be removed after embolization.
A, The smaller balloon is the embolization balloon. It is at the arterial side of the fistula. The larger balloon is the bracing balloon. It is partially inflated now, and will be inflated further to cover the ICA surface of the embolization balloon.
B, The bracing balloon is inflated such that it is large enough to cover the inner surface of the ICA.
C, After deflation and then inflation of the embolization balloon, it is partially inflated and in the CS.
D, The embolization balloon inside the CS is inflated to its proper size to obliterate the fistula. Then, the bracing balloon is deflated and ready to be removed.
fig 4. Lateral-view carotid angiogram after embolization shows disappearance of fistula
For the second situation, we inflated the embolization balloon and brought it inside the CS. Then, the bracing balloon was inflated in the ICA to occlude the opening of the fistula. Next, the embolization balloon in the CS was slowly inflated to a size larger than the opening of the fistula. The remaining procedures were the same as for the above-mentioned step 5 through step 8.
Results
We have performed the double-balloon technique in 11 of 29 fresh CCFs with patent parent ICAs after the standard single-balloon technique failed. In nine of them, the fistulas were successfully obliterated (Table). There were two failures in which the balloon could not pass through the fistula regardless of the maneuver used. In one of them, the fistula was finally explored with a microcatheter and was obliterated by using microcoils and an n-butyl-2-cyanoacrylate (NBCA) mixture inside the CS. In the other case, the fistula became larger and could only be managed by occlusion of the parent ICA. However, no neurologic complication was noted. There were no other complications resulting from this technique.
Discussion
The size of the CS and the fistula may affect the success rate of detachable-balloon embolization of a CCF. The CS must be large enough to accommodate the detachable balloon/balloons for embolization. The size of the fistula must be smaller than the inflated balloon, but large enough to allow access for a deflated or partly inflated balloon. However, the size of the fistula should not be too large, because the embolization balloon may retract to the ICA at inflation in the CS.
Graeb et al (7) suggested the combination of a large fistula with a small CS might preclude safe balloon detachment in the CS. Therefore, precautions must be taken to avoid intraarterial balloon detachment in the treatment of CCF in order to preserve the blood flow in the ICA.
The double-balloon technique is particularly useful for the following two occasions. First, the orifice of the fistula or flow is too small for passage of the deflated or slightly inflated balloon. Second, the width of the CS is smaller than is the opening of the fistula; ie, the combination of a large fistula with a small CS.
In the embolization of a CCF achieved using the detachable balloon/balloons, the balloon is usually carried to the venous side (CS), where the blood flow is. If the orifice of the fistula is small or the flow through the fistula is slow, a detachable balloon may not be carried to the venous side by blood flow. Under this circumstance, it is usually impossible to embolize the fistula and preserve ICA flow with detachable balloon/balloons from an arterial approach without using a special maneuver. Herein we describe a double-balloon technique in which a bracing balloon temporarily occludes the ICA at the orifice of the fistula, facilitating passage of the embolization balloon through the fistula to the CS, in the direction of least resistance. However, the double-balloon technique may also fail if the fistula is really too small. In this situation, other techniques can be used to treat the CCF while preserving ICA flow, such as 1) transarterial catheterization with a microcatheter and embolization with an NBCA mixture or microcoils (10–12) and 2) transvenous embolization through the inferior petrosal sinus or through the ophthalmic vein (13–14). Direct puncture of the CS through the superior orbital fissure is a difficult technique and is not recommended in usual cases of CCF (15).
Occasionally, when the width of the CS is smaller than the opening of the fistula, inflation of the balloon inside the venous side (CS) may push the balloon back to the ICA. By using the double-balloon technique, the embolization balloon inside the CS can be inflated to a size larger than the diameter of the opening of the fistula while the bracing balloon is temporarily inflated in the ICA. Because the embolization balloon is larger than the size of the fistula, it will remain inside the CS after removal of the bracing balloon in the ICA. Another reason that the embolization balloon will stay inside the CS is that, with the help of a bracing balloon, the embolization balloon can adapt to a shallow space in the CS, molding into a disklike shape and occluding the fistula. The double-balloon technique may not always work when the fistula is too large and the CS is too small. Then, occlusion of the parent ICA as well as the fistula may be necessary.
There are several potential risks in applying the double-balloon technique. Overinflation of the bracing balloon in the ICA may result in rupture of the ICA, enlargement of the fistula, or creation of a new CCF. If the bracing balloon is a detachable balloon, it may be detached prematurely while the embolization balloon is inflated. Premature detachment of the inflated bracing balloon in the ICA may eventually result in occlusion of the ICA, because retrieval of the detached balloon is usually very difficult. Patients who cannot tolerate acute occlusion of the ICA will suffer from cerebral infarction. We used a detachable balloon as the bracing balloon because it was readily available to us. We believe a nondetachable occluding balloon, or a double-lumen–occluding balloon, would be a better selection. The following precautions should be emphasized in order to prevent possible premature detachment of the bracing balloon in the double-balloon technique. The bracing balloon should be tied firmly onto the 2F catheter; otherwise, a nondetachable balloon should be used instead. The bracing balloon should be inflated to a size that is large enough to be trapped on the inner wall of the ICA so that it will not be detached during inflation of the embolization balloon. The importance of careful fluoroscopic monitoring during inflation, deflation, and movement of these balloons cannot be overemphasized.
Conclusion
We have described a double-balloon technique for the embolization of CCF. This technique is helpful in the following conditions. 1) The detachable balloon cannot be carried to the CS by blood flow because of the relatively small size of the fistula. 2) The detachable balloon can pass through the fistula, but inflation of the balloon inside the CS pushes the balloon back to the ICA.
Footnotes
↵1 Address reprint requests to Michael Mu Huo Teng, M.D., Department of Radiology, Taipei Veterans General Hospital, 201, Sect 2, Shih-Pai Road, Peitou, Taipei, Taiwan, 11217 Republic of China.
References
- Received June 14, 1999.
- Accepted after revision April 13, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Mid- and long-term outcomes of carotid-cavernous fistula endovascular management with Onyx and n-BCA: experience of a single tertiary center
- Use of Onyx for Transarterial Balloon-Assisted Embolization of Traumatic Carotid Cavernous Fistulas: A Report of 23 Cases
- Treatment of a traumatic carotid-cavernous fistula by the sole use of a flow diverting stent
- Multimodal endovascular therapy of traumatic and spontaneous carotid cavernous fistula using coils, n-BCA, Onyx and stent graft