Abstract
BACKGROUND: When treating acute ischemic stroke due to large-vessel occlusion, both mechanical thrombectomy and intravenous (IV) thrombolysis carry the risk of intracerebral hemorrhage.
PURPOSE: This study aimed to delve deeper into the risk of intracerebral hemorrhage and its subtypes associated with mechanical thrombectomy with or without IV thrombolysis to contribute to better decision-making in the treatment of acute ischemic stroke due to large-vessel occlusion.
DATA SOURCES: PubMed, EMBASE, and Scopus databases were searched for relevant studies from inception to September 6, 2023.
STUDY SELECTION: The eligibility criteria included randomized clinical trials or post hoc analysis of randomized controlled trials that focused on patients with acute ischemic stroke in the anterior circulation. After screening 4870 retrieved records, we included 9 studies (6 randomized controlled trials and 3 post hoc analyses of randomized controlled trials) with 3241 patients.
DATA ANALYSIS: The interventions compared were mechanical thrombectomy + IV thrombolysis versus mechanical thrombectomy alone, with the outcome of interest being any form of intracerebral hemorrhage and symptomatic intracerebral hemorrhage after intervention. A common definition for symptomatic intracerebral hemorrhage was pooled from various classification systems, and subgroup analyses were performed on the basis of different definitions and anatomic descriptions of hemorrhage. The quality of the studies was assessed using the revised version of Cochrane Risk of Bias 2 assessment tool. Meta-analysis was performed using the random effects model.
DATA SYNTHESIS: Eight studies had some concerns, and 1 study was considered high risk. Overall, the risk of symptomatic intracerebral hemorrhage was comparable between mechanical thrombectomy + IV thrombolysis and mechanial thrombectomy alone (risk ratio, 1.24 [95% CI, 0.89–1.72]; P = .20), with no heterogeneity across studies. Subgroup analysis of symptomatic intracerebral hemorrhage showed a non-significant difference between 2 groups based on the National Institute of Neurological Disorders and Stroke (P = .3), the Heidelberg Bleeding Classification (P = .5), the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (P = .4), and the European Cooperative Acute Stroke Study III (P = .7) criteria. Subgroup analysis of different anatomic descriptions of intracerebral hemorrhage showed no difference between the 2 groups. Also, we found no difference in the risk of any intracerebral hemorrhage between two groups (risk ratio, 1.10 [95% CI, 1.00–1.21]; P = .052) with no heterogeneity across studies.
LIMITATIONS: There was a potential for performance bias in most studies.
CONCLUSIONS: In this systematic review and meta-analysis, the risk of any intracerebral hemorrhage and symptomatic intracerebral hemorrhage, including its various classifications and anatomic descriptions, was comparable between mechanical thrombectomy + IV thrombolysis and mechanical thrombectomy alone.
ABBREVIATIONS:
- AIS
- acute ischemic stroke
- HBC
- Heidelberg Bleeding Classification
- HI
- hemorrhagic infarction
- ICH
- intracerebral hemorrhage
- IVT
- intravenous thrombolysis
- LVO
- large-vessel occlusion
- MT
- mechanical thrombectomy
- PH
- parenchymatous hematoma
- RCT
- randomized clinical trial
- sICH
- symptomatic ICH
Since the release of a series of influential randomized clinical trials (RCTs) in 2015, followed by a patient-level meta-analysis in 2016, the combination of mechanical thrombectomy (MT) and intravenous thrombolysis (IVT) has been recognized as the primary treatment for eligible patients with acute ischemic stroke due to large-vessel occlusion (AIS-LVO).1
IVT offers certain advantages, such as earlier treatment initiation and possibly increasing the chance of reperfusion of the occluded vessel.2 However, it may also increase the risk of intracerebral hemorrhage (ICH) and other bleeding-related complications.3,4 Therefore, several RCTs have been conducted to assess the benefits and safety of adding IVT to MT in eligible patients with AIS-LVO. However, the risk of ICH following combined MT and IVT (MT+IVT) continues to be a debatable subject in the literature due to the inconsistency of the results of RCTs.5,6
A recent meta-analysis of 6 RCTs by Majoie et al7 reported a lower incidence of any ICH in the MT alone group, but no difference in symptomatic ICH (sICH). Prior meta-analyses also showed a non-significant difference between MT+IVT and MT alone in terms of sICH.2,8 This observation calls for a more detailed investigation, including an examination of hemorrhage subtypes using various criteria. In this article, we present a novel meta-analysis that addresses the safety profiles of MT alone versus MT+IVT for AIS-LVO. Unlike previous reviews, our study meticulously evaluated various definitions of sICH and examined hemorrhage subtypes. Additionally, we incorporated recent evidence that was not included in prior systematic reviews. Thus, this study aimed to compare the risk of hemorrhage and its subtypes between MT and MT+IVT. By doing so, we aimed to enhance our understanding of these treatment strategies and provide valuable insights for clinical decision-making.
MATERIALS AND METHODS
This systematic review and meta-analysis was conducted in accordance with the guidelines set forth by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).1 In addition, the study was registered in advance with a specified review protocol in PROSPERO, under the registration number CRD42023478018.
Search Strategy
We searched PubMed, Embase and Scopus databases spanning all records from inception to September 6, 2023. The search syntax was developed by a combination of relevant keywords and medical subheadings (MeSH) including stroke, cerebral infarction, thrombectomy, endovascular therapy and hemorrhage. In the search process, there was no language, country, or date limitation for inclusion of the reports. The full search strategy is available in the Online Supplemental Data. In addition, the references of the articles that passed the full-text screening were manually examined to retrieve any potentially missed articles.
Eligibility Criteria
Only randomized clinical trials or the post hoc analysis of RCTs that satisfied our population, intervention, comparison, and outcome criteria were eligible to include. The population was patients with AIS in LVO in the anterior circulation. The intervention/comparison was MT+IVT versus MT alone. The outcome of interest was the bleeding risk after intervention in terms of any type of ICH (any ICH), sICH, or the anatomic description of hemorrhage within brain. We excluded observational studies, conference abstracts, and reviews. Only systematic reviews were retained, and their references were manually checked.
Selection Process
Two authors (S.B.J. and L.H.) screened the titles and abstracts independently on the basis of predefined criteria. In case of any disagreement, another author (S.G.) was consulted to reach consensus. The full texts of all abstracts that met the inclusion criteria and reference checking of systematic reviews were assessed independently by the same 2 authors.
Data Extraction
An Excel-based data extraction sheet (Microsoft) was created by 1 author (C.B.). It contained study characteristics, baseline data of the patients included, and the outcomes of interest. Afterward, 2 authors (S.B.J. and L.H.) conducted a pilot extraction. The results of the pilot extraction were reviewed by 2 authors (C.B. and S.G.), and the form was revised to prevent any prior mistakes. All articles were reviewed independently by 2 authors (S.B.J. and L.H.). Any discrepancies or disagreements were resolved through discussion and consensus.
Risk of Bias
Two independent reviewers (S.B.J. and L.H.) assessed the quality of all studies using the revised version of Cochrane Risk of Bias 2 assessment tool (https://methods.cochrane.org/risk-bias-2). This tool classifies 5 domains of bias into the following categories: 1) selection bias, which arises from random sequence generation and allocation concealment; 2) bias due to deviations from intended interventions; 3) attrition bias, which arises from missing outcome data; 4) bias in the measurement of the outcome; and 5) bias in selective reporting of results.
Statistical Analysis
To have a common definition for sICH between studies, we pooled sICH definitions with a common criterion of neurologic deterioration as evidenced by an increase of ≥4 points on the NIHSS from baseline and evidence of ICH on follow-up imaging within 24–48 hours from intervention. By using this definition, we pooled data of sICH defined by the Heidelberg Bleeding Classification (HBC), the European Cooperative Acute Stroke Study III (ECASS III), Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST), and sICHsite. The definition of each classification system is available in the Online Supplemental Data. We also ran a subgroup analysis on different definitions if there were ≥2 studies in each sICH definition. Another subgroup analysis was performed to assess the risk of hemorrhage at different anatomic descriptions used by the studies. These anatomic descriptions included hemorrhagic infarction (HI), HI1, HI2; parenchymatous hematoma (PH), PH1, PH2; subarachnoid hemorrhage (SAH); and interventricular hemorrhage.
All analyses were conducted using R software, Version 4.3.2 (http://www.r-project.org) meta package Version 6.5–0 (https://cran.r-project.org/web/packages/meta/index.html) and metafor package Version 4.4–0. (https://cran.r-project.org/web/packages/metafor/index.html). We calculated the risk ratios and their corresponding 95% CIs using the random effects model to pool the data. Heterogeneity was assessed using the Q statistic and the I2 test, in which I2 > 50% or P < .05 was considered significant.9 The Egger regression test was used to assess the publication bias, with P < .10 considered significant.10 In the case of significant heterogeneity, a sensitivity analysis was performed with the removal of outlier studies to bring the heterogeneity to an insignificant level. Outlier studies were identified using the method previously described by Viechtbauer and Cheung.11
RESULTS
Search and Screening Results
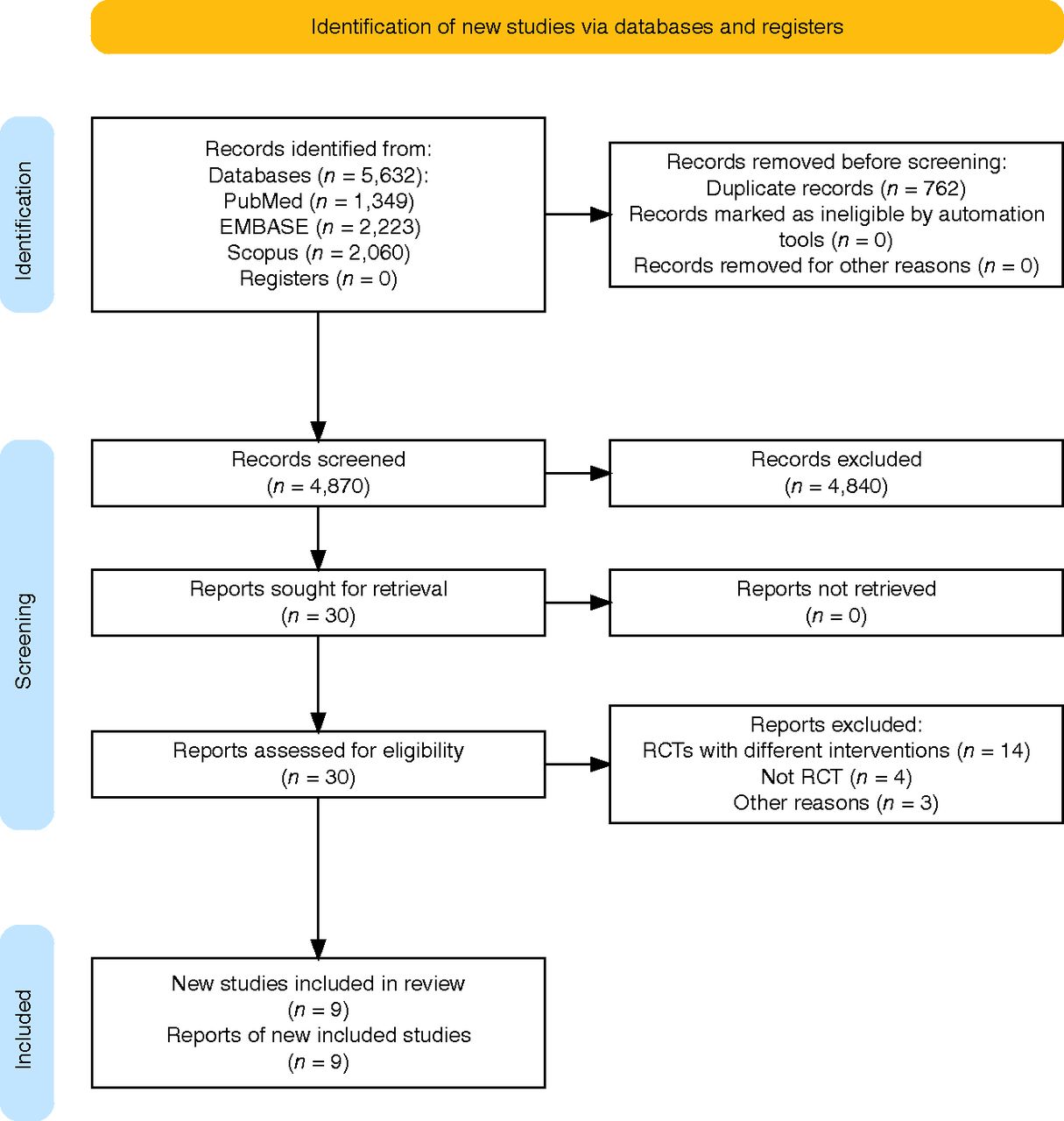
Following the removal of 762 duplicate records, 4870 articles were retrieved for further screening. Through the title and abstract screening stage, 4840 records were excluded and 30 records were retained for full-text screening. An additional study was identified via expert recommendation. Finally, 9 studies12⇓⇓⇓⇓⇓⇓⇓-20 were determined to satisfy the inclusion criteria with the appropriate report of outcomes of interest (Fig 1).

PRISMA diagram detailing the literature search process.
Study Characteristics and Risk of Bias
Six RCTs13,15⇓⇓⇓-19 and 3 post hoc analyses of RCTs12,14,20 were included. Demographic information about these studies is presented as Online Supplemental Data. Overall, the studies included 3241 patients, of whom 1490 received MT alone and 1751 patients received MT+IVT. Most patients were men, comprising 1741 individuals (53.7%). The dose of IVT was 0.9 mg/kg in all studies except Direct Mechanical Thrombectomy in Acute LVO (SKIP) (0.6 mg/kg). All studies excluded posterior circulation strokes except the DIRECT-SAFE (A Randomized Controlled Trial of DIRECT Endovascular Clot Retrieval versus Standard Bridging Thrombolysis with Endovascular Clot Retrieval within 4.5 Hours of Stroke Onset) trial, which included 19 patients (6.5%) with basilar stroke and post hoc analyses of the COMPASS (Aspiration Thrombectomy versus Stent Retriever Thrombectomy as First-Line Approach for Large Vessel Occlusion) trial and Solitaire With the Intention for Thrombectomy (SWIFT) and Solitaire Flow Restoration Thrombectomy for Acute Revascularization (STAR) trials, which included <1% posterior occlusions. The SITS-MOST criteria were used in 4 studies, HBC and ECASS III criteria were used in 3 studies, and NINDS (National Institute of Neurological Disorders and Stroke) criteria was used in 2 studies. One study used sICHsite and sICHglobal criteria to define sICH.
Eight studies had some concerns mostly arising from deviations from the intended interventions (performance bias), and 1 study was high risk. This study was a post hoc analysis of the combination of a single-arm study (STAR) with a randomized clinical trial (SWIFT) and was regarded as high risk due to the high probability of missing data and randomization. Details of risk of bias assessment are available in the Online Supplemental Data.
Any ICH.
Pooled analysis of 8 studies containing 2942 patients showed a comparable risk of any ICH between MT and MT+IVT groups (risk ratio, 1.10 [95% CI, 1.00–1.21]; P = .052). There was no heterogeneity across studies (I2 = 0.0%, P = 1) (Fig 2).

Meta-analysis with a random effects model shows a comparable risk of any ICH between MT and MT+IVT. ASTER indicates Contact Aspiration versus Stent Retriever for Successful Revascularization; RE, Random Effects; DEVT, A Randomized, Controlled, Multicenter Trial of Direct Endovascular Treatment versus Standard Bridging Therapy for Acute Stroke Patients with Large Vessel Occlusion in the Anterior Circulation; MR-CLEAN NO-IV, Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands–NO IV.
sICH.
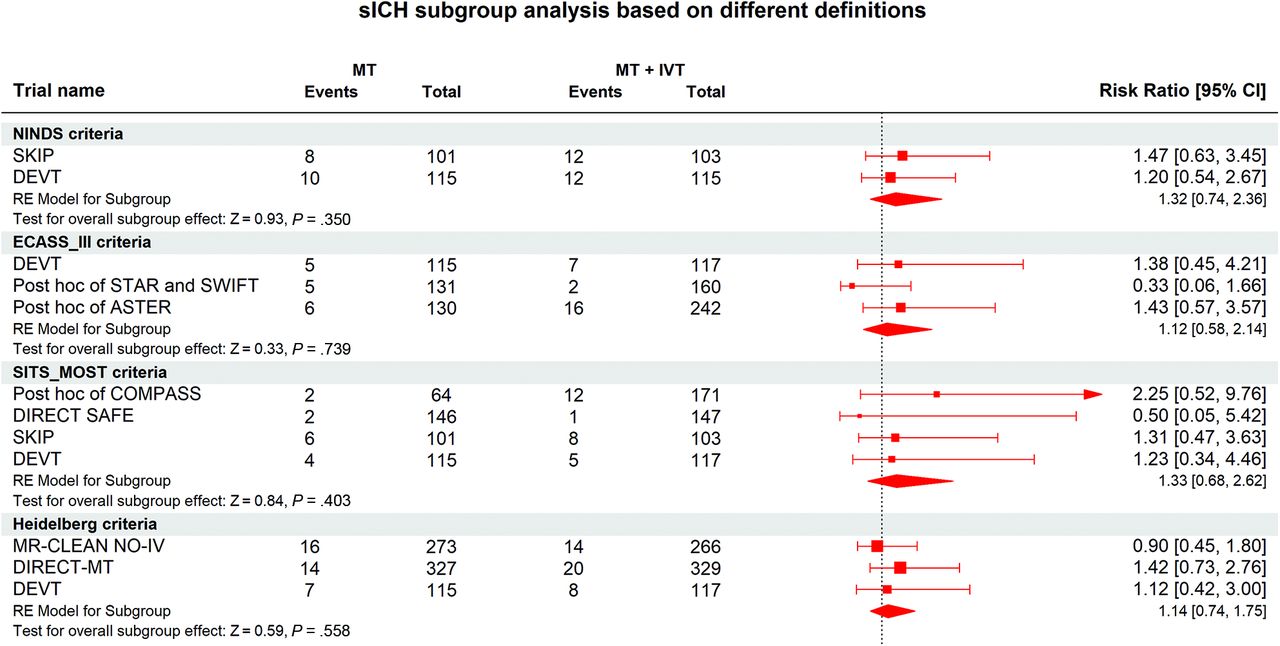
Pooled analysis of 9 studies containing 3227 patients showed no difference between risk of sICH between 2 groups (risk ratio, 1.24 [95% CI 0.89-1.72]; P = .20). There was no heterogeneity across studies (I2 = 0.0%, P = .52) (Fig 3). Subgroup analysis of sICH based on NINDS, HBC, SITS-MOST, and ECASS-III criteria also showed a non-significant difference between MT+IVT versus MT groups (Fig 4).

Meta-analysis with random effects shows a comparable risk of symptomatic ICH between MT and MT+IVT. DEVT indicates A Randomized, Controlled, Multicenter Trial of Direct Endovascular Treatment versus Standard Bridging Therapy for Acute Stroke Patients with Large Vessel Occlusion in the Anterior Circulation; ASTER, Contact Aspiration versus Stent Retriever for Successful Revascularization; MR-CLEAN NO-IV, Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands–NO IV.

Subgroup analysis of different symptomatic ICH definitions shows no difference between MT and MT+IVT. DEVT indicates A Randomized, Controlled, Multicenter Trial of Direct Endovascular Treatment versus Standard Bridging Therapy for Acute Stroke Patients with Large Vessel Occlusion in the Anterior Circulation; ASTER, Contact Aspiration versus Stent Retriever for Successful Revascularization; RE, Random Effect. MR-CLEAN NO-IV, Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands–NO IV.
Anatomic Description of Hemorrhage.
Subgroup analysis of different anatomic descriptions of ICH is presented in Fig 5. There was no difference between the MT+IVT and MT groups in any descriptions.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subgroup analysis of different symptomatic ICH anatomic descriptions shows no difference between MT and MT+IVT in the risk of hemorrhage at shown anatomic levels. MR-CLEAN NO-IV indicates Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands–NO IV; SWIFT-DIRECT, Solitaire With the Intention For Thrombectomy Plus Intravenous t-PA versus DIRECT Solitaire Stent-Retriever Thrombectomy in Acute Anterior Circulation Stroke; DEVT, A Randomized, Controlled, Multicenter Trial of Direct Endovascular Treatment versus Standard Bridging Therapy for Acute Stroke Patients with Large Vessel Occlusion in the Anterior Circulation; ASTER, Contact Aspiration versus Stent Retriever for Successful Revascularization.
DISCUSSION
Our meta-analysis included 9 studies (6 RCTs and 3 post hoc analyses from RCTs) with a total of 3241 patients. Our results showed that there were no statistically significant differences between IVT+MT and MT alone in terms of any ICH and sICH. In a meta-analysis of 3 RCTs, Du et al,21 reported a higher risk of any ICH in MT+IVT and suggested using MT without IVT. Likewise, Majoie et al7 reported a lower risk of any ICH in the MT-alone group (OR, 0.82; 95% CI, 0.68–0.99), However, our analysis revealed a similar risk between the 2 treatment groups. This discrepancy is noteworthy, and we attribute it to the increased statistical power of our study due to a larger sample size (2942 versus 2313 patients in the analysis of any ICH risk). In terms of ICH subtypes, Hu et al4 reported a higher occurrence of PH in patients treated with MT+IVT in a secondary analysis of the DIRECT-MT (Direct Intraarterial Thrombectomy in Order to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals: A Multicenter Randomized Clinical Trial) trial. This result highlights the need to explore different subtypes of ICH in other trials. In our analysis, there were no differences between the 2 treatment modalities in any category of the anatomic description of the hemorrhage. To the best of our knowledge, our study is the first study that examines different anatomic subtypes of hemorrhage among RCTs comparing MT versus MT+IVT.
The use of IVT in addition to MT in eligible patients with AIS-LVO has been investigated in many studies including a few RCTs and several observational studies. On the one hand, IVT might facilitate successful recanalization of LVO via its lytic effect on the occlusive clot being rendered easier to extract by MT.22,23 Moreover, animal studies suggest that IVT might have beneficial pleotropic effects on the CNS that extend beyond its fibrinolytic effect.24 On the other hand, the use of IVT might be associated with an increased risk of ICH.25 Also, there is a counterargument that the lytic effect of IVT on the occlusive clot is not necessarily always beneficial, given that it might make the clot more likely to fragment during the MT procedure, leading to distal microembolism,26,27 which is associated with worse outcomes.28
While several studies and meta-analyses looked into the comparison between IVT+MT and MT alone in terms of clinical benefits and safety profile, there are a few factors that need to be further studied regarding this comparison. For example, the collateral status is thought to be associated with a decreased risk of ICH after MT;29 thus, the risk of ICH with IVT+MT needs to be studied in patients with a good collateral status versus those with a poor collateral status. Also, the location of the LVO within the anterior circulation versus the posterior circulation should be considered while conducting such a comparison. Another factor that needs to be further investigated is the size of the ischemic stroke in patients undergoing IVT+MT.30 The impact of pretreatment cerebral microbleeds on the outcomes of MT in patients with AIS-LVO was reported not be associated with increased risk of ICH in a recent meta-analysis,31 which did not include a subgroup analysis according to adjunctive IVT use with MT. Therefore, the effect of pretreatment cerebral microbleeds on IVT+MT outcomes should be studied in future RCTs. Last, regarding the MT procedure itself, there are a few factors that should be considered for subgroup analyses in future RCTs comparing IVT+MT with MT alone. These factors include but are not limited to the MT technique (stent retriever versus direct aspiration),32 the use of adjunctive treatments,28,33 and performing acute carotid stent placement during the MT procedure, given the need for immediately starting those patients on antiplatelet therapy.34
Our research is not without its limitations. First, certain patient-specific attributes may influence the risk of ICH. Unfortunately, we lacked access to data on these individual characteristics. For instance, the use of preprocedural aspirin or heparin was associated with elevated sICH risks in the MR CLEAN MED trial.35 However, we were unable to harmonize the usage of antiplatelet or anticoagulant agents across different studies. Second, factors such as the baseline NIHSS, ASPECTS, occlusion site, comorbidities, and reperfusion status play pivotal roles in predicting post-MT ICH.36,37 While these parameters are typically balanced within treatment arms of individual RCTs, pooling data from diverse studies may affect the results. Furthermore, we pooled different sICH definitions into 1 category to analyze sICH. However, even with a logically-derived definition, subtle variations across sICH definitions can introduce heterogeneity.
CONCLUSIONS
Our meta-analysis revealed that there were no statistically significant differences between MT alone and MT+IVT in terms of any ICH and symptomatic ICH. Future research should evaluate the collateral status of patients, the location of the LVO within the anterior or posterior circulation, the size of the ischemic stroke, the impact of pretreatment cerebral microbleeds, and specific factors related to the patients or the MT procedure itself. This result will help to fully comprehend the influence of various factors on the outcomes of these treatment strategies in AIS-LVO.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- Received March 7, 2024.
- Accepted after revision April 1, 2024.
- © 2024 by American Journal of Neuroradiology