
Abstract
BACKGROUND AND PURPOSE: Although the thymus is centered in the mediastinum, often a cervical component can be seen in children and young adults. The frequency of radiologically evident residual cervical thymus in older adults is not known. The purpose of our study was to determine the proportion of adults who have residual cervical thymus visible on contrast-enhanced neck CT.
MATERIALS AND METHODS: We retrospectively identified 700 patients who had undergone contrast-enhanced CT between February 2013 and August 2013. We categorized the patients by decade of life and calculated the proportion in which residual cervical thymic tissue could be detected. The location of the tissue focus, greatest axial diameter, and distance above the manubrium were recorded. A multivariate model was used to determine whether age or sex predicted the likelihood of identifiable cervical thymus, the size of residual thymus, or the distance of residual thymus above the sternum.
RESULTS: Of the 700 patients, 157 (22.4%) had residual cervical thymus. The mean distance of the residual thymus above the manubrium was 13.4 ± 7.26 mm. The mean size of the residual cervical thymus was 12.5 ± 4.11 mm. The frequency of residual thymus decreased exponentially with age. There was a statistically significant relationship between age and the size of the residual cervical thymus (P = .02). Most of the cervical thymic tissue was found in the left paratracheal region.
CONCLUSIONS: Residual cervical thymus may be present at any age, though the frequency decreases with increasing age.
Although the thymus is centered in the superior mediastinum, frequently a radiologically detectable cervical component of the gland can be seen in children and young adults.1 This cervical extension can mimic a pathologic mass or enlarged lymph node, potentially leading to unnecessary surgery and increased medical costs. Radiologists are often unaware of residual cervical thymus tissue as a normal finding, not only in the pediatric population but also in the adult population, because no comprehensive study of residual cervical thymus has been conducted on adults, to our knowledge.
We hypothesized that radiologically detectable residual cervical thymus is present throughout patients' lives and that the frequency of detectable residual cervical thymus decreases with age. The purpose of this study was to determine the proportion of adults at various ages in whom residual thymic tissue can be detected superior to the level of the sternum on CT.
Materials and Methods
Subjects
The institutional review board at the University of Pittsburgh Medical Center approved this retrospective study of existing imaging data, and written consent was waived. We retrospectively searched our electronic medical records to identify contrast-enhanced CT scans of the neck obtained between February 2013 and August 2013, each performed on a different adult patient.
Patients were grouped into 10-year age intervals based on their age (in years) at the time of the examination. The 7 groups were 20–29 years, 30–39 years, 40–49 years, 50–59 years, 60–69 years, 70–79 years, and 80 years and older. Exactly 100 patients were included from each group; once 100 patients in a group were accumulated, no further patients from that group were evaluated. The criterion for inclusion was a contrast-enhanced CT that included the superiormost extent of the manubrium and the lower neck. Patients were excluded if they had undergone surgery or radiation to the lower neck, if the scans demonstrated malignancy within the lower neck or enlarged lower cervical lymph nodes, if there was edema in the lower neck soft tissues, if there was inadequate scan coverage of the neck, or if streak artifacts prevented clear evaluation of the lower neck.
Imaging
CT was performed on a 64-channel scanner (LightSpeed; GE Healthcare, Milwaukee, Wisconsin) with variable milliampere and kilovolt(peak) of 120. Display FOV varied with patient size but was approximately 25 mm; coronal and sagittal reformats were not used in this evaluation.
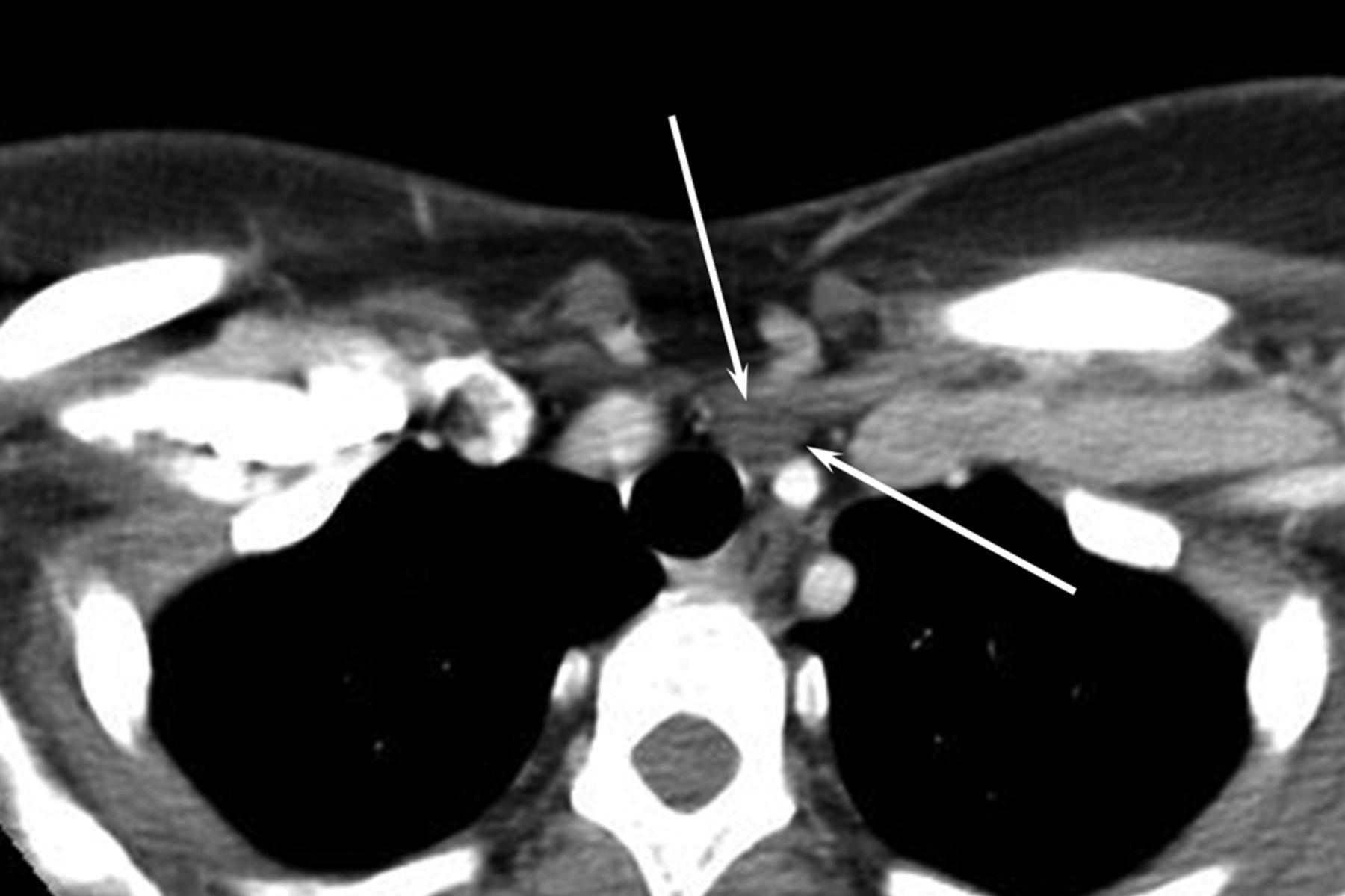
Each examination was evaluated by 1 of 2 Certificate of Added Qualification–certified dedicated head and neck radiologists (B.F.B. and H.A.K., with 12 and 8 years of experience, respectively) to determine whether residual cervical thymic tissue was present. Thymic tissue was defined as an oval focus of soft tissue interspersed with fat that had CT texture similar to that of the mediastinal thymus (Fig 1). The mass had to be discrete and well-defined (we chose this criterion to be conservative and avoid overcalling residual thymus). Only foci above the sternal notch were considered cervical. In patients with residual cervical thymus, the location of the tissue focus, size (greatest axial diameter), and distance between the midpoint of the tissue and the upper border of the manubrium were recorded.

Axial contrast-enhanced CT image through the lower neck shows a uniform, well-defined ovoid mass (arrows) with mixed fat and soft-tissue elements deep to the sternal head of the sternocleidomastoid muscle. This is the characteristic location and appearance of residual cervical thymus.
Statistical Tests
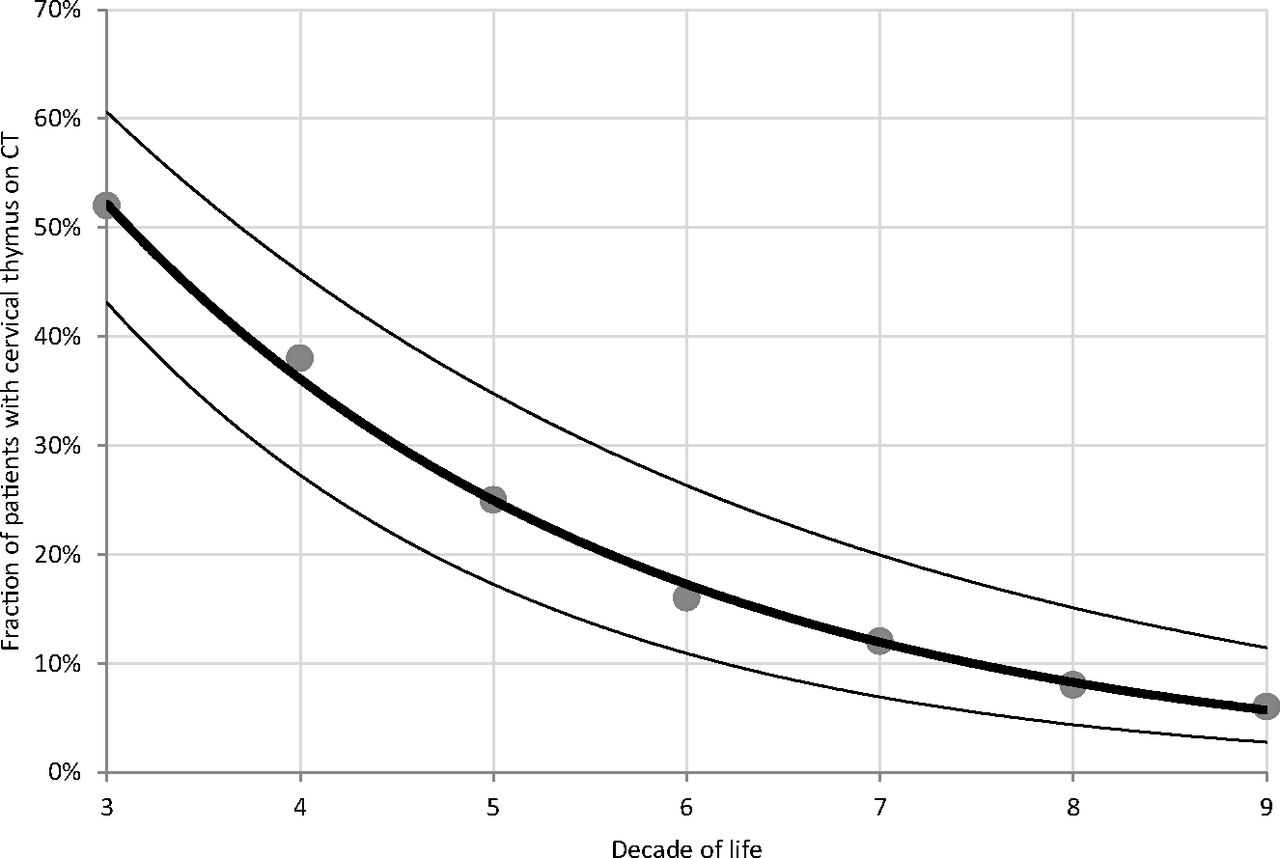
Patients were grouped by decade of age. The percentage of patients with residual cervical thymus in each age group was tabulated and graphed, and a least-squares logistic regression curve was applied (Fig 2). A multivariate model was used to determine whether age or sex predicted the likelihood of identifiable cervical thymus, the size of the residual thymus, or the distance of the residual thymus above the sternum. All tests were 2-sided, and a P value of .05 was chosen as the threshold for statistical significance. SPSS, Version 22 (IBM, Armonk, New York) was used for all statistical calculations.

Graph demonstrating the relationship between the age decade and the presence of the cervical thymus on CT. Circular markers are raw data. The dark line is best-fit logistic regression. Thin lines are 95% confidence intervals. The third decade of life indicates patients 20–29 years of age.
Results
The 700 studied patients included 338 male (48.3%) and 362 female patients (51.7%). Of the 700 patients, 157 (22.4%) had residual cervical thymus. The mean distance of the residual thymus above the manubrium was 13.4 ± 7.26 mm. The mean size of the residual cervical thymus was 12.5 ± 4.11 mm.
The frequency of residual cervical thymus by 10-year age intervals is depicted in Table 1. Residual cervical thymus was seen in all decades of life. The frequency declined from 52% in the third decade of life to 25% in the fifth decade of life to 6% in the ninth decade of life. Residual cervical thymus was found in the left paratracheal region in 108 (69%) of 157 patients (Table 2).
Frequency and size of residual cervical thymus visualized on neck CTa
Location and frequency of residual cervical thymusa
Multivariate analysis demonstrated a statistically significant relationship between age and the size of the residual cervical thymus (P = .02, Table 1). There was no statistically significant relationship between sex and frequency or between sex and size of the residual cervical thymus. There was also no statistically significant relationship between age and the distance of the residual thymus above the manubrium or between sex and the distance of the residual thymus above the manubrium.
Discussion
On CT in adults, the normal thymus can be seen as a triangular-shaped structure in the anterior mediastinum,2⇓–4 reflecting apposition of the 2 thymic primordia that arose from diverticula in the third branchial pouches. As age increases, the thymus undergoes normal involution in which mediastinal fat replaces glandular tissue.5 Wide variability in thymic size and morphology, coupled with its association with diverse pathologic processes, allows the thymus to occasionally mimic pathology.2⇓–4,6
Our study demonstrates that residual thymic tissue in the neck is a commonly occurring variant of the normal thymus, which should not be mistaken for pathology. In our study, residual cervical thymus was present throughout all decades of life. Of the 700 patients, 157 (22.4%) had residual cervical thymus, with approximately two-thirds of the thymus located in the left paratracheal region. Residual cervical thymus was evident in more than half of the patients in their 20s and showed an exponential decay in frequency with increasing patient age. Although the most common location for cervical thymic tissue is in the left paratracheal region, it can be seen anywhere in the lower neck.
This study builds on the work of Costa et al,1 who determined the frequency of the residual cervical thymus in pediatric patients. They showed superior cervical extension of the thymus in 133 (66.5%) of 200 patients, ranging from zero to ≥20 years of age, with a mean age of 9.0 years.1 Our results are consistent with the concept of cervical thymus as a frequent, normal anatomic finding. Together, these studies paint a complete picture of the presence and frequency of the cervical thymus in the pediatric and adult populations.
The differential diagnosis for a low-attenuation mass in the lower neck includes an enlarged Virchow node, thyroid mass, parathyroid mass, paratracheal lymphadenopathy, thymic cyst, and enlarged distal thoracic duct.7 Cervical thymus may be distinguished from these entities by the CT texture (lobules of soft tissue interspersed with fat), which is similar to the texture of the native thymus.6
The decreased frequency of the residual cervical thymus with age is most likely the result of the natural involution of the gland.5 However, other explanations could be offered. The distance between the thyroid gland and the sternum decreases with age, so that thymic tissue that was cervical in young adulthood could become retrosternal in later life. In addition, obesity can cause lower neck structures to shift into the thorax, potentially forcing the cervical thymus under the sternum. However, the consistent distance between the sternum and the cervical thymus across our patient population suggests that involution is the best explanation.
Residual cervical thymus should not be confused with ectopic cervical thymus.8⇓⇓⇓–12 Ectopic cervical thymus is the result of aberrant embryology. The thymus is derived from the paired third pharyngeal pouches in the upper neck. The thymic primordia descend via the thymopharyngeal ducts, which normally involute. Residual cells along this pathway may develop into ectopic foci of thymic tissue.13,14 These ectopic foci can appear anywhere along the line from the angle of the mandible to the thyroid gland.15 Ectopic thymic tissue is more common in males and is usually on the left side.9,16,17 In contrast, the residual cervical thymus is continuous with the mediastinal thymus during childhood and becomes disconnected by selective atrophy of portions of the gland.
Our study has some important limitations. The study was retrospective, and all patients in the study were imaged for varying clinical reasons. Sick patients might have a higher rate of visible residual cervical thymus, but this is acceptable because it reflects the actual rate of cervical thymus that would be seen on medical imaging. The observers interpreting the images were blinded to patient age, but their clinical experience allowed them to gauge the approximate age of each patient on the basis of the images, which could have introduced bias. Finally, there was no histologic confirmation of the residual thymic tissue, but we think that the predictable decline in frequency of this finding with age reinforces our conclusion that this is indeed the thymus.
Conclusions
Residual cervical thymus may be present at any age and should not be mistaken for pathology. Residual cervical thymus is most frequently encountered in the left paratracheal region.
Acknowledgments
The authors thank Rose Jarosz for her role as research coordinator for this study.
References
- Received November 23, 2014.
- Accepted after revision December 29, 2014.
- © 2015 by American Journal of Neuroradiology





{kind=link}
{kind=link}